Endoscopic Spine Systems
Spine Endoscopy Equipment from elliquence
Endoscopic Spine Surgery is gaining in popularity among clinicians looking to improve outcomes and patient satisfaction.
elliquence®, LLC, is the leading expert of Radio Wave Solutions with the Surgi-Max® Ultra RF Generator and the original Trigger-Flex® directional RF handpiece. Together now with simple, smart, and comprehensive Endoscopic Spine Systems, elliquence offers clinicians the full ability to perform endoscopic procedures with approaches for Transforaminal, Interlaminar, Rhizotomy, and Spinal Stenosis.
Endoscopy Technology for Spine Conditions & Surgery
Our endoscopic spine technology allows medical professionals to safely and efficiently perform endoscopic procedures to treat spine conditions. Whether you are a spine surgeon at a hospital or a doctor in your own practice, our endoscopy equipment can help you treat a range of spinal conditions and injuries, such as disc herniations.

Transforaminal Endoscopy
Endoscopic Facet Denervation
elliquence Endoscopic Instrumentation
Endoscopes
Avialable for all approaches

Dilators / Coaxial Step Dilators
Available in a variety of sizes

Graspers
Available in a variety of types and sizes


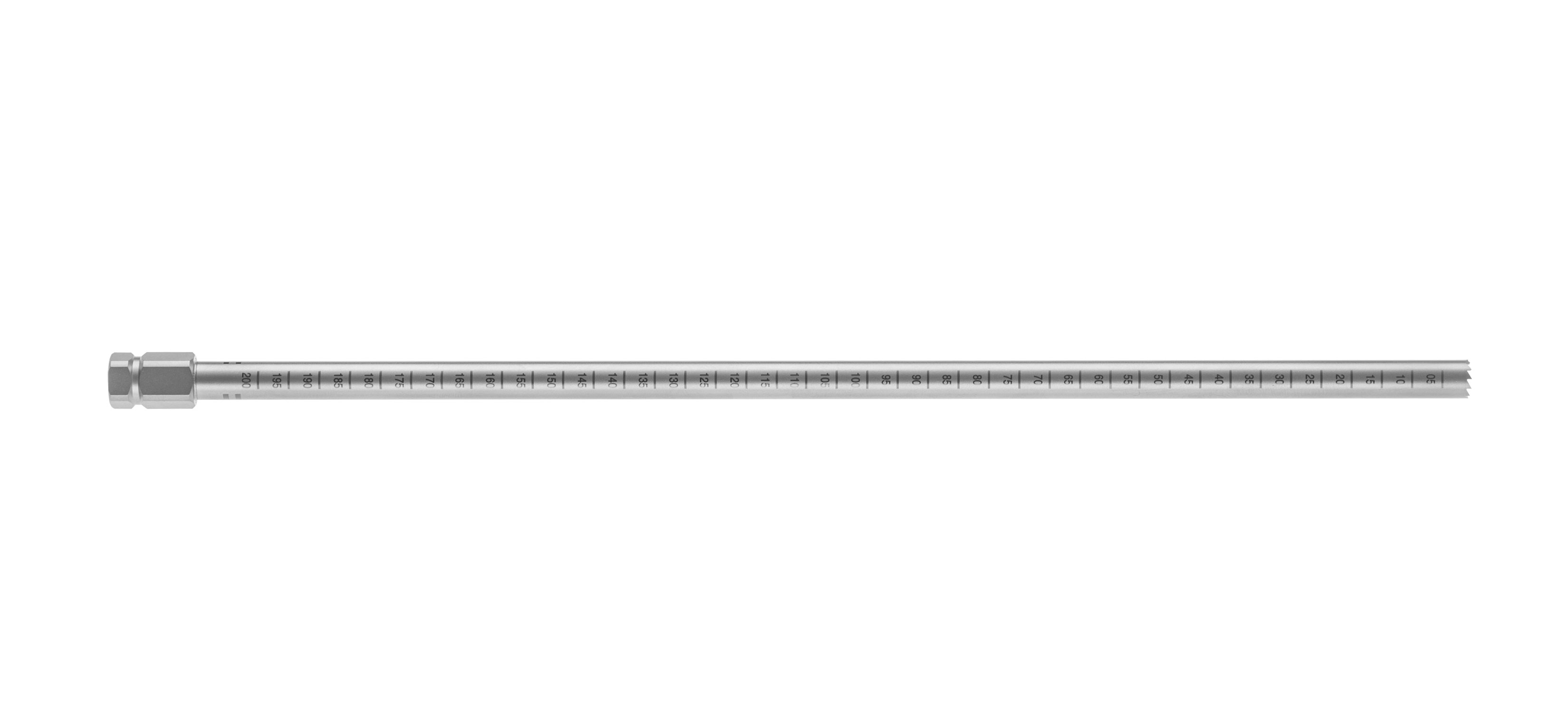
Working Tubes
Available in various sizes and types



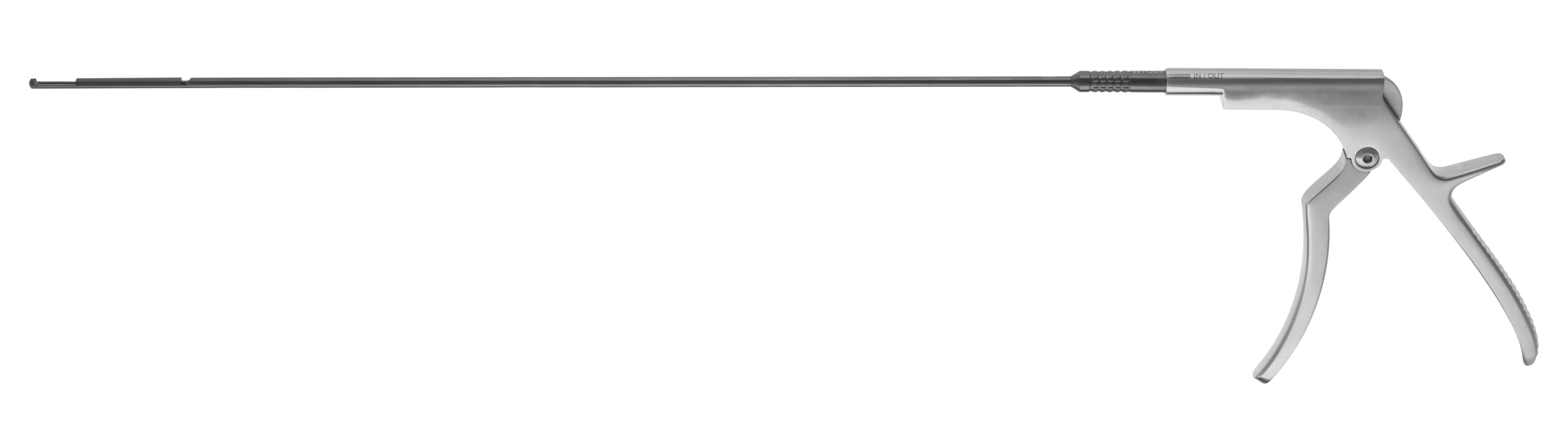
Kerrisons


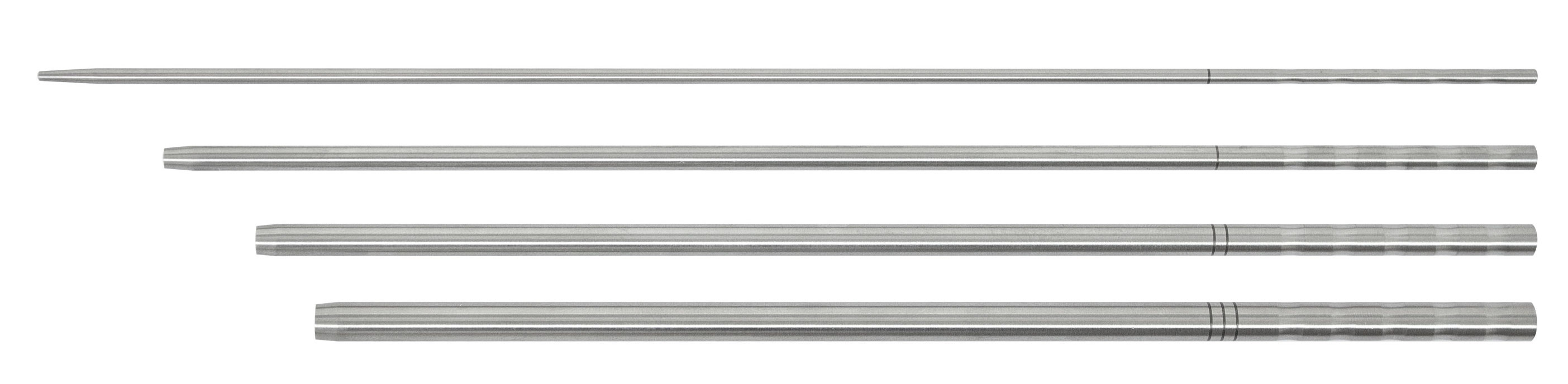
Trephines

Incorporate elliquence Medical Technology Today
Endoscopic spine surgery is a minimally invasive procedure that surgeons perform to treat a range of spine conditions. Our Endoscopic Spine Systems help medical professionals treat patients quickly and efficiently with minimal scarring and recovery time. Contact elliquence online or call us at 516-277-9000 today to discuss to learn more about how you can implement our Endoscopic Spine Systems.
Gun Choi, MD
elliquence technology
“An important consideration for anyone doing endoscopic surgery is how to ablate tissue and create hemostasis. Not all methods are created equal and I have found over the last 15 plus years that elliquence’s technology is trustworthy and performs better than other RF machines, allowing me to achieve better results. elliquence technology cleanly and efficiently ablates the tissue while controlling hemostasis very effectively, and as a result is a key component in excellent patient outcomes.”

Nicholas Prada, MD
Approach on Interlaminar
The interlaminar window at L5-S1 is easily accessed through a direct posterior approach, visualized using both AP and Lateral radiographs. The lateral facet is located and the stab incision is made directly medial to the facet to the level of the fascial layer. The dilator is introduced to the level of the ligamentum flavum, confirming AP and Lateral radiographs. The cannula is introduced over the dilator with the bevel open medially and the endoscope is introduced. Various instruments including the Trigger-Flex® RF probe are used to expose the ligamentum flavum. Punches and kerrisons can now be used to perforate the ligamentum for access to the spinal canal. The nerves are visualized and mobilized using a dissector. The canula is rotated to further mobilize, retract and protect the nerves exposing the herniation. A variety of instruments along with the Trigger-Flex® RF probe can now be utilized to remove disc material. The small wound site can be closed with minimal suture or steri-strips.

Jim Yue, MD
Approach on Transforaminal
Patient selection is critical to the success of any surgical approach, the herniated disc tissue must be accessible through the foramen. Patient is positioned in the prone position on either bolsters or a Wilson frame to open up the foraminal space. AP and Lateral radiographs are used to identify the targeted foraminal levels. If an intra-discal approach is elected, an 18 gauge spinal needle is initially introduced not past the medial edge of the pedicle AP view, and in the posterior 3rd of the disc space in the lateral view with care being taken to avoid the exiting nerve root. The guide wire is transferred through the needle and a stab incision is performed along the guide wire. The dilator is introduced over the guide wire to the level of the annulus, again care should be taken to avoid the exiting nerve. The beveled cannula is introduced over the dilator creating a working portal for the introduction of the endoscope for direct visualization, light, irrigation and working access to the previously identified pathology. Upon completion of the surgery, the small wound can be closed with either steri-strips or a single stitch.

Jorge Ramirez, MD
Approach on Rhizotomy
Endoscopic Dorsal Ramus Rhizotomy is a procedure that can provide patients with relief of pain associated with degenerative disease of the facet joints. Use of the spine endoscope provides visualization of the posterior spinal anatomy and nerves, while an endoscopic RF probe facilitates the ablation of the medial (and lateral) branches of the dorsal ramus and can lead to more complete ablation of the nerves and therefore better and longer lasting pain relief. Endoscopic Rhizotomy is most effective in those patients who have experienced greater than 50% relief of pain with medial branch blocks. The Endoscopic Dorsal Ramus Rhizotomy procedure offers an alternative for addressing axial back pain that is much less invasive than spinal fusion. A Rhizotomy is primarily done at the junction where the medial branch of the dorsal ramus nerve crosses over the transverse process of the vertebral body, however to make sure a complete ablation is accomplished rotating the RF probe through a full 360˚ ensures a complete evulsion of the nerves is achieved.

Stefan Hellinger, MD
Approach on Stenosis
Lumbar spinal stenosis is a common cause of radicular and generalized back pain among older adults. Endoscopic minimally invasive surgery, in contrast to open decompression, may provide the opportunity for a less invasive surgical intervention. Visualization and illumination during the operation can be optimized. Since a more extensive bone or ligament resection is frequently necessary here, a larger diameter endoscope with a correspondingly larger endoscopic working channel and larger instruments and burrs are necessary. After the access has been created, the bony structures are exposed. It may be helpful to start decompression at the caudal end of the descending facet. Depending on the pathology, decompression is then commenced with resection of parts of the medial descending facet, the cranial and caudal lamina, and the ligamentum flavum. The extent of decompression generally continues cranially at least until the tip of the ascending facet and caudally to half of the pedicle. The medial portions of the ascending facet and the ligamentum flavum are then resected until sufficient decompression of the neural structures can be clearly seen. In the case of a central stenosis, the ligamentum flavum generally needs to be resected medially to the midline. If the patient experiences bilateral symptoms of stenosis, an “over the top” access using the undercutting technique to the opposite side is carried out.